Children who walk on their toes, even though they can, on request, walk with their entire foot down, are referred to as idiopathic toe walkers. There should be no other cause for toe walking, and it should arise in connection with the initiation of walking. For most children, toe walking is not a problem, and many stop walking on their toes during preschool years, sometimes a bit later after starting school. The treatment of children with ITW is not aimed at the toe walking itself but the problems that may arise if the child has a shortened Achilles tendon, becomes weak in the muscles, or has reduced motor skills compared to children of the same age. If a child is lagging behind in motor skills, motor training is needed – it is crucial for being able to participate in play with peers. If mobility is reduced, the child may need to be assessed by an orthopedic specialist and potentially undergo Achilles tendon lengthening. If the child is weak in the muscles, strength training may be necessary. If the child has good function, full mobility, and strength, then toe walking is not a problem. A physiotherapist can regularly follow up with the child to ensure that they maintain mobility, strength, and motor function.
ITW-guide
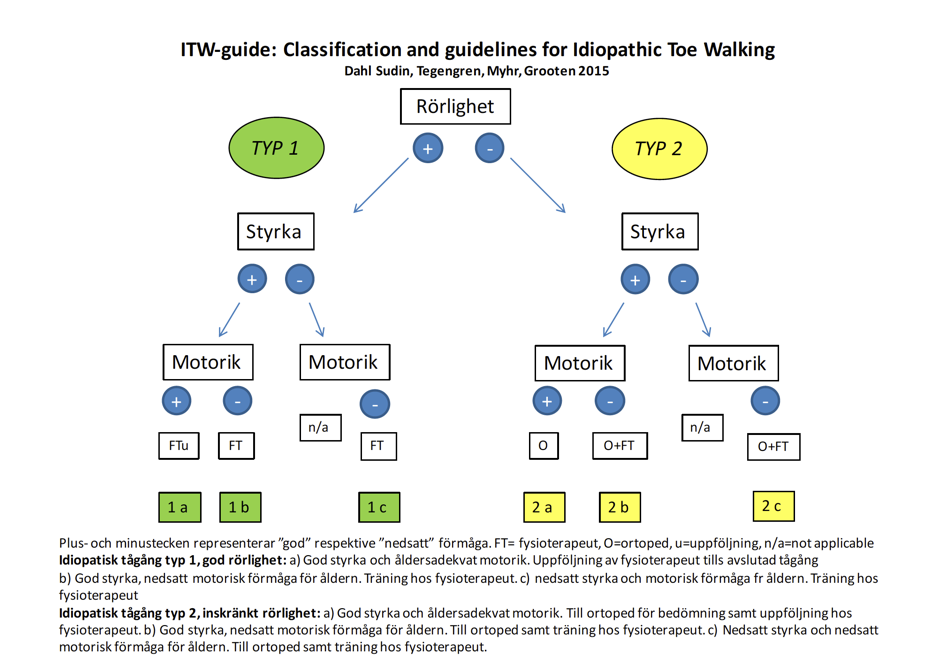
The ITW guide is a flowchart that categorizes children with ITW into 2 types depending on whether they have reduced mobility or not. Further classification regarding strength and motor skills is done, and recommendations for follow-up, training, or assessment by a physiotherapist or orthopedic specialist are provided depending on the child’s clinical presentation. The ITW guide helps streamline healthcare by identifying which authority the child should be referred to. The ITW guide is a result of clinical reasoning based on research on strength measurements in children with ITW and motor skill training for children with ITW. It was presented at the Physiotherapy Days in Stockholm 2015.
Flowchart for the treatment/follow-up of children with ITW.
Containers baby syndrome (CBS) is a relatively new term developed by child specialists, referring to a collection of movement, behavioral, and other issues caused by a baby or infant spending too much time in a common ‘container’ used in the child’s daily life. Examples include car seats, strollers, Bumbo seats, vibrating chairs, baby sitters, baby rockers, nursing pillows, sleep sacks, standing supports, or baby walkers. Although these items provide comfort, give parents time to attend to siblings or other tasks, and to some extent entertain the child, they hinder the child’s ability to explore their surroundings. The inability to explore the environment directly impacts the child’s motor skills, language, cognitive development, and can cause structural deformities. The good news is that container baby syndrome can be prevented 100 percent!
These items can make parents believe that they create safety, simplicity, and a contented child – and that something is wrong if the child is sad or protests against having to exert effort with their body. There is a lack of knowledge and information about the fact that the frustration a child may show is the very drive and signal for learning – and that parents need to understand that they should have high expectations for the child’s ability to learn to control their body. Instead of thinking something is wrong, the parent needs to encourage and stimulate the child towards ACTIVITY and DEVELOPING IN TUMMY TIME. Many parents are content with the child sitting up, claiming that the child is comfortable and does not want to lie on their stomach. It is important to understand that sitting requires significantly fewer of the foundational skills developed in crawling. Crawling is more demanding than walking and develops strength, mobility, and balance skills that the child needs. It should be easy for the child to lift their body against gravity and move around while crawling. When a child learns to move around, they often become happier and start exploring their surroundings.
Sitting ‘lying down’ without supporting the body.
The term ‘sittvagn’ has gained a new meaning and implies passive sitting.
The term ‘sittvagn’ has gained a new meaning and implies passive sitting.
Consequences of CBS
Allows little or no activity in the body – neck, spine, and extremities.
If you’re wondering if your child is ready to ride a bike or how to help create the conditions for cycling, you can watch this video that provides practical tips for preparing for cycling.
Consequences of too much supine positioning – on babies back
Newborn babies are currently recommended to sleep on their backs, as supine positioning has clearly reduced the incidence of sudden infant death syndrome. This is encouraging and positive. Parents are informed that babies should lie on their stomachs during awake time, but sometimes the advice is vague, and it does not explain WHY the baby should lie on their stomach and WHEN they should start. Studies from the USA and Canada show that more than 25% of parents are so afraid of sudden infant death syndrome that they do not place the baby on their stomach, even though they know they should. A new problem of inactivity has arisen where completely healthy babies acquire motor difficulties already during the newborn period. The babies are too passive, and when they are passive for too long, there is a risk of developmental problems and lack of stimulation of basic functions that should occur at a certain time.
We have known for some time that there is a “window of opportunity” when the newborn’s eye muscles should start working and the eyes should stop squinting. If squinting continues into later stages, the child may develop vision impairment due to the fact that the visual center in the brain did not develop at the right time. We are not certain whether or how different aspects of motor development are affected by supine positioning, such as how the programming of the balance organs is affected by lack of head lifting, how the development of hand function is affected by hands not being loaded against the floor, or how the development of coordinated leg movements and muscle strength is affected when the newborn does not perform crawling movements. However, research shows that the overall development of the child is negatively affected by passivity during the newborn period. In Sweden, there is limited research on the consequences of how supine positioning affects motor basic functions and the overall development of the child. In countries like the Netherlands, Canada, and the USA, there are clearer measures in place, and they monitor the consequences that arise from babies sleeping on their backs and having reduced time in prone position.
Asymmetric head shapes
Nearly half of Swedish infants today have an asymmetric skull shape, which affects neck function and also the entire body’s motor skills. Sometimes, the child has a symmetric but pointed shape when lying on their back without turning their head to one side. A newborn’s head is proportionally larger than that of an adult. The child has been bent in the womb and lacks full mobility in certain joints When the child lies on their back on a flat surface, the head is large, and the whole body is unstable, often causing the head to fall to one side. It is difficult for the child to bring their head back to the opposite side as it becomes heavy and lacks the support of a pillow. Since the skull bones are not fused, the unilateral pressure leads to one side of the skull becoming flat, and the ear and forehead on the flat side protrude in relation to the opposite side. The head shape becomes asymmetrical. The neck muscles on one side are activated while those on the other side are not triggered, leading to weakness.
Head shape asymmetry should ideally be prevented and, if not, early treated by having the child lie and load the “round” side of the head through positioning. Head shape asymmetry regresses with mechanical loading of the non-flat side. If the child continues to load only one side, the skull asymmetry will increase. A pediatric physiotherapist can assess and monitor skull asymmetry and guide parents to ensure that the child achieves a good skull shape.
Pictures: Asymmetric head shape, also called Plagiocephaly.
Neck
In a child’s development, the first thing to learn is to hold the head straight and the eyes in the horizontal plane. This occurs as receptors in the neck, eyes, and ear balance organs synchronize. In prone position, the child lifts the head from side to side, the eyes move before the neck, and the lift activates the semicircular canals in the ear. The child learns to turn the head right and left and gains both passive and active mobility in the neck. The child loads cheeks and hands, performs weight transfers, develops the ability to activate neck muscles, and begins to develop eye-hand coordination. Quite soon, the child can hold the head straight and gaze forward. When a child lies only on the back, none of this happens, and they become weak and tilt the head. One side of the neck is strong, and the other is weak or inactive – the child does not “find out” how to start and activate the neck muscle. This resembles the inactivation of eye muscles that do not stop squinting. Children who squint need tasks to start the eye muscles. The same goes for the neck, and it is good to start during the child’s first month of life. By the age of 2-3 months, the child should have developed “optical balance reaction” (see film clip 2) which is a coordination of the eye and neck that allows the child to hold up the head and eyes even if the body leans. Sometimes parents delay placing the child on the stomach until they are 3 months old. When suddenly placed on the stomach and unable to lift the head, the child often protests and begins to cry. Parents may then feel sorry for the child and think something is wrong, and therefore pick up the child. The child is often placed in a walker, another chair, or stroller. It is common for the child to lack optical balance reaction on one side of the neck and hold the head tilted to one side. A strong and capable child often becomes a happy and content child. A weak child becomes frustrated and sad. Physical well-being is linked to mental health already during infancy.
In normal motor development, you can expect that:
The child can lift the head from side to side in prone position during the neonatal period.
By 2-3 months of age, the child should have developed optical balance reaction.
At 3 months, the child should be able to lie on the stomach, lift the head, and alternate between forearm and hand support.
Between 3 and 6 months, the child should move around its own axis sideways.
During the third quarter, the child learns to crawl or move forward.
Experienced physiotherapists in clinical practice often encounter a pattern that was less common in the past. This pattern shows a lack of arm and hand strength, weakness in the back and neck, impaired balance, and delayed motor development. Sometimes, the child continues to tilt their head to one side even after they start walking. Often, these children have used baby walkers or have sat with rounded backs on backward-leaning seats, which makes it impossible to maintain a straight back and neck.
Knowledge and interventions are needed to counteract both skull asymmetries and delayed activation of the neck, as well as the passivity and deterioration of infant development. Advice on neck exercises needs to be clearer and initiated as early as the neonatal period.
For those who wish to read more, here is a reference list that can be a starting point, although it does not claim to be exhaustive.
Tilted neck, eyes slanting.Straight neck, eyes in a straight line.
For those who are pediatric nurses, pediatricians, or pediatric physiotherapists, this film will provide you with insights into children’s motor development from 0 to 2 years, as well as deeper understanding in areas such as skull asymmetry, foot and leg development, and the impact of strollers on sitting posture. This educational film is suitable for anyone working with children, including parents. It provides knowledge that fosters confidence and strategies for knowing when to react and take action if a child is delayed. About the film: The film focuses on the first two years of a child’s motor development. It describes the developmental stages that children go through and highlights the factors influencing their development. Eight children and a preschool group illustrate how children learn everything from crawling to running and jumping. The film also includes in depth discussions about skull asymmetries in babies, foot and leg development, and how strollers affect a child’s sitting posture. Total length 28 minutes.
Children need tasks to solve in order to develop, as well as a good environment – both physical and psychological. Here is the introduction to the film about motor development 0-2 years. Let babies be active 🙂
This film describes the Optic Balance Reaction, something learned between 2 and 3 months of age and retained throughout life.
Here is some information about 1 year motor development and the difference between dynamic and static balance, as well as how your feedback to the child affects their self-esteem.
Here is an introduction to asymmetrical skulls – they should be prevented – more facts are available in the film about motor development 0-2 years.
Vi använder cookies för att se till att vi ger dig den bästa upplevelsen på vår webbplats. Om du fortsätter att använda denna webbplats kommer vi att anta att du godkänner detta.